Home Based Vision Therapy For Children – Part 2
This is the continuation of the article ‘Home Based Vision Therapy For Children Part 1’ where we were informed about Vision Therapy.
In the previous article (Home Based Vision Therapy For Children – Part 1) we had covered the 4 Home Based Vision Therapies as mentioned below below
- Pencil Push Up Test
- Stereogram
- Brock String
- Life Saver Card
To continue, we will now explore the other options.
5. Therapy For Oculomotor Dysfunction And Accommodation Dysfunction
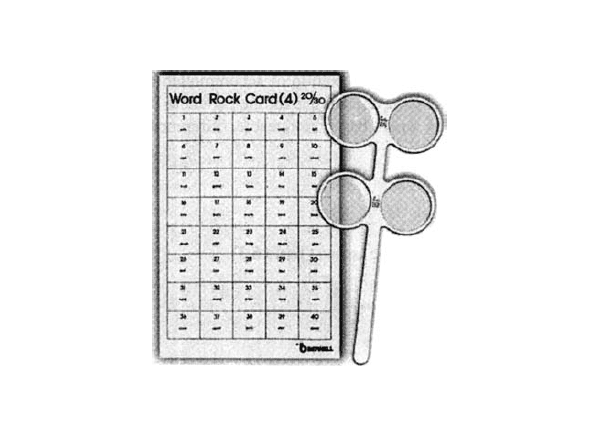
a) Accommodative Flippers
Purpose
Flippers (powers range from +/-2.00D down to +/-1.00D) help to improve accommodative facility – The ability to increase and decrease focusing demand.
Procedure
While looking through one side of your flippers read one word of the reading chart. Try to keep each word clear as you read it aloud. Flip it over so you are looking through the other side of the lenses. Read the next word aloud. Flip back to the first set of lenses and read the next word.Repeat this process until your each the bottom or cannot focus well enough to read the words. Try to do 1 minute of flipper reading, and then give yourself 30 seconds rest. Repeat 5 cycle do these 3 times a day.
b) Hart Char Distance to Near Accommodative Rock (Monocular)
Purpose
The objectives of Hart chart rock are to restore normal accommodative amplitude and facility. Both the range over which the patient can accommodate and the speed of the accommodative response are considered important in this technique.
Equipment Needed
Large Hart chart suitable for distance viewing,Small Hart chart suitable for near viewing.
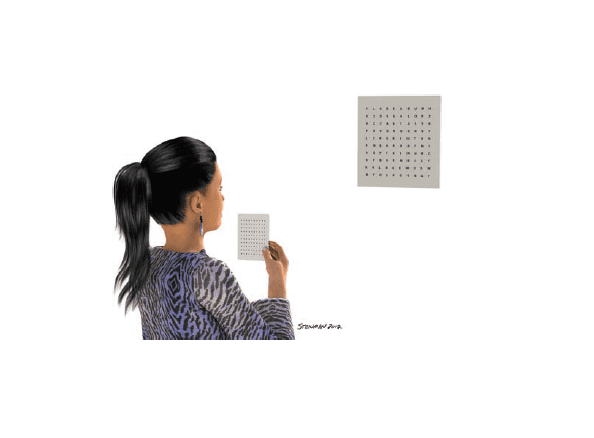
Procedure
a. Cover patient’s left eye with the eye patch. Patient holds the small chart at 40 cm, and focus on the top line, read the line when it is clear. After reading the top line on the near chart, ask him or her to look at the second line of the far Hart chart and read it when it is clear. The patient continues to alternate from the near to the far Hart chart for several minutes. Repeat the entire sequence with the right eye covered and the left eye open.
b. Ask the patient to hold the small chart at arm’s length and to call off the letters on the top line,patient slowly moves the chart closer. When the patient can no longer keep it clear, have him shift to the second line of the larger chart, which is placed at about 10 ft. Have the patient repeat the procedure with the third line of the small chart, moving it closer as patient calls off the letters. Repeat the procedure with the patch moved to the right eye.
c. To increase the level of difficulty, ask the patient to hold the near chart 1 to 2 in. farther away than the point at which he or she reports blurred vision and switch fixation from the larger distance chart to the smaller near chart. Each time the patient switches fixation, he or she reads a line.
Endpoint
For patients younger than 20 years, discontinue this therapy technique when the patient is able to successfully clear the near chart when it is held 3 in. from his or her eyes and then change fixation and clear the far Hart chart held at 10 ft. For patients older than 20, the endpoint depends on the amplitude of accommodation. Discontinue this procedure when the patient can successfully clear the near chart, which is held at a distance equal to half of his or her amplitude.
c) Saccadic Therapy
Only distance hart chart is used.
6. Paper Pencil and Miscelleanous Tasks
For special population and with learning disabilities. This category includes training techniques that are printed on paper and designed to train vergence, accommodation,Amblyopia (with Patching) and accurate eye movements.
7. Computer Orthoptics
Computer-assisted vision therapy involves activities that stress vergence, eye movements, accommodation and visual information processing.
a) Home Therapy System
HTS, includes one saccadic and one pursuit technique. The HTS vergence program optometrist has option to monitor the patient’s performance at home and modify program when necessary over the Internet. In addition, this company has developed two other home-based programs that are specifically designed to treat eye movement disorders. The first is called Perceptual Visual Tracking Program and includes five computer procedures designed to improve saccadic accuracy and speed (Matching Targets, Moving Box, Moving Line , Hidden Targets, Saccadic Tracking).
- Moving Text Dynamic Reading: The material to be read remains in the center of the screen and does not move down the page from top to bottom; therefore, saccadic eye movements are not required.
- Standard Dynamic Reading: The print moves left to right and top to bottom. The reading rate starts at a level that should be comfortable for the patient. It increases as the patient progresses.
- Whole Line Dynamic Reading: The material to be read does not move left to right but is presented as an entire line at a time. The reading material moves down the page one line at a time to the end of the passage. A reading fluency test determines the starting words per minute (WPM) for the patient. A major benefit of all of these home-based therapy programs is the ability to monitor the patient’s compliance over the internet.
b) Computer-Aided Vision Therapy: Track and Read
Computer-Aided Vision Therapy has home therapy programs for binocular vision, eye movement, and visual information processing therapy. The program that is found useful for home-based vision therapy for eye movements is called Track and Read.
Special Note On Tips for Vision Rest
Individuals who spend lengthy periods focusing on computer screens should follow the 20/20/20 rule. This suggests resting your eyes after 20 minutes of computer use for at least 20 seconds while looking at an object that’s 20 feet away. A comprehensive eye exam with a reliable eye doctor, however, allows you to explore different eye protection options.
Conclusion
To get the effective and desired result, following things need to be maintained:
- The Vision Therapy must be easy to use.
- The purpose & procedure must be well explained by Optometrist and properly understood by patients& guardians.
- High Motivation from both patient and the parents, is of great value.
References:1. Cooper, J. (2007). Computerized vision therapy for home and office treatment of accommodative disorders, vergence disorders, and amblyopia. Journal of Behavioral Optometry, 18(4), 88.2. Vision Therapy: The best kept secret and its role for children with specialneedsMarie L. Fox, OD kalamazoovalleyeyecare.com3. Natasha Huffine, M. S., OTRL, C., & Kara Christy, M. S. Vision Therapy: Beyond Compensations and Addressing the Root of the Problem.4. VISION AND LEARNING GUIDE By COVD.5. Chapter 8 of Office-Based Vision Therapy (VT/Orthoptics).6. Clinical Management of Binocular Vision By Mitchell Scheiman & Bruce Wick.