This post is also available in:
![]() العربية
العربية
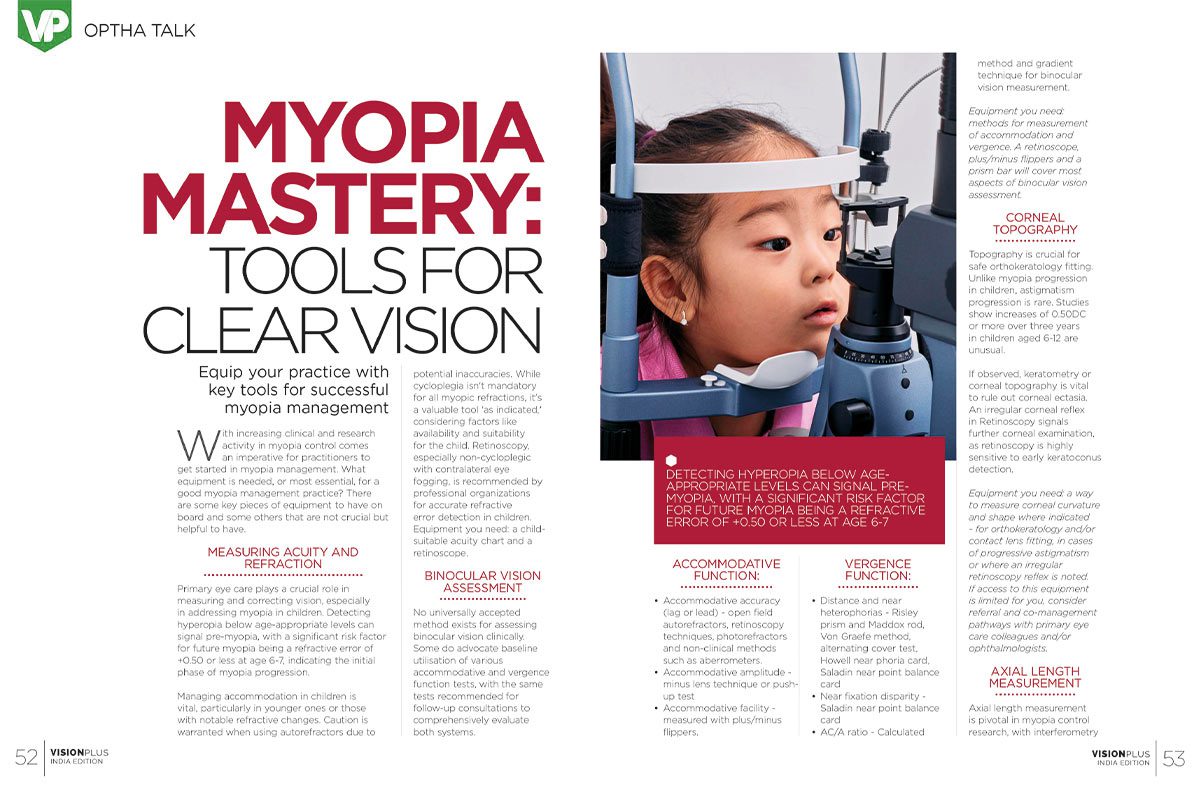
Myopia Mastery: Tools For Clear Vision
Equip your practice with key tools for successful myopia management
With increasing clinical and research activity in myopia control comes an imperative for practitioners to get started in myopia management. What equipment is needed, or most essential, for a good myopia management practice? There are some key pieces of equipment to have on board and some others that are not crucial but helpful to have.
Measuring Acuity And Refraction
Primary eye care plays a crucial role in measuring and correcting vision, especially in addressing myopia in children. Detecting hyperopia below age-appropriate levels can signal pre-myopia, with a significant risk factor for future myopia being a refractive error of +0.50 or less at age 6-7, indicating the initial phase of myopia progression.
Managing accommodation in children is vital, particularly in younger ones or those with notable refractive changes. Caution is warranted when using autorefractors due to potential inaccuracies. While cycloplegia isn’t mandatory for all myopic refractions, it’s a valuable tool ‘as indicated,’ considering factors like availability and suitability for the child. Retinoscopy, especially non-cycloplegic with contralateral eye fogging, is recommended by professional organizations for accurate refractive error detection in children. Equipment you need: a child-suitable acuity chart and a retinoscope.

Binocular Vision Assessment
No universally accepted method exists for assessing binocular vision clinically. Some do advocate baseline utilisation of various accommodative and vergence function tests, with the same tests recommended for follow-up consultations to comprehensively evaluate both systems.
Accommodative Function:
- Accommodative accuracy (lag or lead) – open field autorefractors, retinoscopy techniques, photorefractors and non-clinical methods such as aberrometers.
- Accommodative amplitude – minus lens technique or push-up test
- Accommodative facility – measured with plus/minus flippers.
Vergence Function:
- Distance and near heterophorias – Risley prism and Maddox rod, Von Graefe method, alternating cover test, Howell near phoria card, Saladin near point balance card
- Near fixation disparity – Saladin near point balance card
- AC/A ratio – Calculated method and gradient technique for binocular vision measurement.
Equipment you need: methods for measurement of accommodation and vergence. A retinoscope, plus/minus flippers and a prism bar will cover most aspects of binocular vision assessment.
Corneal Topography
Topography is crucial for safe orthokeratology fitting. Unlike myopia progression in children, astigmatism progression is rare. Studies show increases of 0.50DC or more over three years in children aged 6-12 are unusual.
If observed, keratometry or corneal topography is vital to rule out corneal ectasia. An irregular corneal reflex in Retinoscopy signals further corneal examination, as retinoscopy is highly sensitive to early keratoconus detection.
Equipment you need: a way to measure corneal curvature and shape where indicated – for orthokeratology and/or contact lens fitting, in cases of progressive astigmatism or where an irregular retinoscopy reflex is noted. If access to this equipment is limited for you, consider referral and co-management pathways with primary eye care colleagues and/or ophthalmologists.

Axial Length Measurement
Axial length measurement is pivotal in myopia control research, with interferometry being 10 times more accurate than refraction for tracking myopia progression.
While not widely adopted in primary eye care, newer instruments and research suggest its potential as a standard.
Measurements, especially with noncontact devices, are recommended, and an axial length beyond 26mm indicates increased risk. As a relative measure, normal growth is about 0.1 mm/yr, while 0.2 to 0.3 mm/yr suggests myopia progression. Future assessments may involve percentile growth charts, comparing a child’s measurement to age-specific data.
Those in the 75th percentile or higher face heightened myopia risk. A decrease in percentile indicates successful myopia management. Understanding axial length dynamics aids proactive myopia strategies and lifelong eye health management.
Equipment you need: ideally, a way to access axial length measurement for your myopic patients, and non-contact (interferometry) methods are most accurate.
Consider co-management with suitably equipped colleagues and/or ophthalmologists to gain measurements, even if only annually, as this extra data can indicate long-term eye health risk and influence management.
Retinal Examination And Imaging
Annual retinal examination, particularly for high myopes and as needed for others, is crucial, conducted through dilated pupils. Optical coherence tomography (OCT) or fundus photos are used to objectively document retinal features or abnormalities when findings emerge. In countries where this technology is commonplace, it might be deemed the standard for myopia care, advocating for annual eye health examinations for all myopes, where feasible.
Equipment you need: it will depend on your scope and setting of practice. Whether you are undertaking the retinal health examination or referring to ophthalmology, ensure your high myopes have a full retinal health examination annually, and low-to-moderate myopia as indicated by your professional standards.
There is more than enough evidence now that doing nothing to control myopia – continuing to fit single vision corrections in progressing childhood myopes – is not the standard of care.
Remember that every dioptre matters in controlling myopia, so stay up to date and get started using the tools and guidance available to you.
Source: Myopia Profile